| Dominant Left Coronary Artery |
| In 8% of cases the left coronary artery (LCA) is dominant because it gives of the postero-lateral artery (PLA) and then travels to the cross-section of the AV groove and the posterior inter-ventricular (IV groove) where it gives rise to the left posterior descending coronary artery (PDA) that travels in the posterior IV groove and gives off several septal perforator branches (SP). The SP supply blood to the lower portion of the IV septum. The dominant LCA also gives rise to the AV nodal branch which supplies blood to the AV node. In about 7% of patients there is a co-dominant or balanced circulation in which case the RCA gives rise to the PDA and then terminates while the Cx artery gives rise to all the postero-lateral (PLA) branches. The Cx may also give rise to a left PDA that runs parallel to the PDA of the RCA. The sinus or sino-atrial (SA) node branch originates in the proximal portion of the RCA in 60% of cases and as a left atrial branch of the Cx in the remaining 40% of cases. This is unrelated to whether a specific artery is "dominant" or not.
The video on the left (below) shows a dominant left coronary artery system. Click the buttons to toggle between the RAO and LAO projections. You can also use the buttons to see a labeled freeze frame. |
|
FOR AUDIO: Click the Speaker Icon to "unmute" Audio 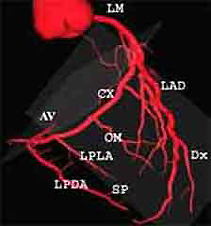 |
  |

| Legend: LM=Left main; LAD=Left anterior descending: Dx=Diagonal; SP=septal perforator; Ramus=ramus intermedius; Cx=Circumflex; OM=Obtuse marginal LPLA=Left postero-lateral branch; LPDA=Left posterior descending artery; AV=AV nodal branch |
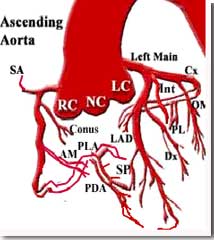
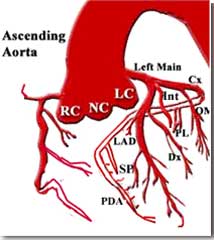
| The diagram on the right (above) shows a dominant left coronary
artery (LCA) system, as described in the previous screen, while the diagram
on the left shows a non-dominant LCA system. Note that the latter supplies
the postero-lateral (PL) branch but does not continue on to the AV groove
to supply the posterior descending artery (PDA), as seen in the dominant
LCA system on the right. |
| Dominant Left Coronary Artery |