| Left Coronary Artery RAO View 1 |
|
|
|
FOR AUDIO: Click the Speaker Icon to "unmute" Audio 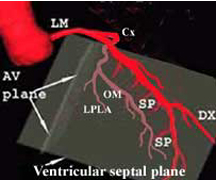 |
 |

| In the RAO view, the LAD begins
close to the spine and then moves away from it and towards the LV apex.
It gives off two sets of branches (one or more diagonals and several septal
perforators). The diagonal (Dx) moves diagonally and away from the LAD. The septal perforators (SP) are smaller branches that come off the inferior border of the LAD (at roughly 90 degrees) and travel downward. The Cx, in this view, moves parallel to the spine and give off the obtuse marginal (OM) and left postero-lateral (LPLA) branches that come off at an angle and run roughly parallel to the LAD. When you have completed review of this screen, please click the "Next page" blue arrow for the second portion of this section. |
| Left Coronary Artery RAO View 1 |