| Right Coronary Artery AP View 1 |
|
In the early days of cardiac catheterization, The x-ray tube, image intensifier and camera remained stationary, while the patient lay in a cradle that was rotated from the RAO to the LAO projections. Cranial and caudal angulation were not possible at those times. These "straight" AP view is limited because the density of the spine interferes with the quality of the angiogram. However, it may be of occasional value in displaying the origin and shaft of the RCA. The right coronary artery (RCA) arises from the anterior position of the right coronary cusp and travels in the anterior atrio-ventricular (AV) groove. Often, the AV groove is seen as a translucent stripe that gives a clue to its location. The conus branch is usually the first branch, and it travels to the right ventricular (RV) outflow tract. Occasionally, the conus artery may have a separate origin from the RCA. |
|
FOR AUDIO: Click the Speaker Icon to "unmute" Audio 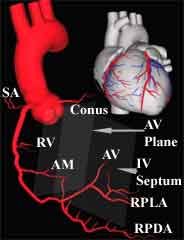 |

| In 85% of cases the RCA travels to the cross-section of the
AV groove and the posterior inter-ventricular (IV groove). At this point,
it gives rise to the right posterior descending coronary artery branch
which travels in the posterior IV groove and gives rise to several septal
perforator branches (SP). The SP supply blood to the lower portion of
the IV septum.
When the RCA supplies the posterior descending coronary artery, as it does in about 85% of cases, it is referred to as a "DOMINANT" RCA. in the other 15% of cases, the circumflex coronary artery supplies the PDA and is then called a "LEFT DOMINANT" coronary artery. The RCA also gives rise to the AV nodal branch which supplies blood to the AV node and the right postero-lateral (RPLA) branch which supplies the lower postero-lateral portion of the left ventricle. When you have completed
review of this screen, please click the "Next page" blue arrow for
the second portion of this section.
|
| Right Coronary Artery AP View 1 |