| Cardiac Cath 3/6 |
 Cardiac
Cath Procedure: After discussing the risk-benefit ratio of the procedure
and obtaining signed informed consent, the patient is brought to the cardiac
or heart catheterization laboratory and placed on the table. Mild conscious
sedation is commonly used and varies according to the preference of the
cardiologist. Intravenous sedation may also be used intermittently during
the case, as needed. Oxygen saturation is constantly monitored.
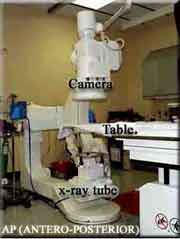
The x-ray tube is attached to one end (on top) and the image intensifier
(II)/camera assembly (below) is attached to the other end of a mobile
arm that can be rotated left and right plus cranially and caudally (towards
and away from the patient's head). This ability allows the patient's coronary
angiograms to be reviewed from various angles. Cardiac
Cath Procedure: After discussing the risk-benefit ratio of the procedure
and obtaining signed informed consent, the patient is brought to the cardiac
or heart catheterization laboratory and placed on the table. Mild conscious
sedation is commonly used and varies according to the preference of the
cardiologist. Intravenous sedation may also be used intermittently during
the case, as needed. Oxygen saturation is constantly monitored.
The x-ray tube is attached to one end (on top) and the image intensifier
(II)/camera assembly (below) is attached to the other end of a mobile
arm that can be rotated left and right plus cranially and caudally (towards
and away from the patient's head). This ability allows the patient's coronary
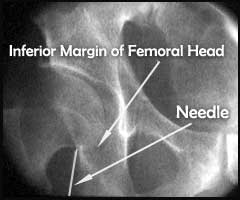
angiograms to be reviewed from various angles.The vascular access site (groin in the majority of cases) is cleansed with an antibacterial solution and covered with surgical drapes. Before proceeding any further, many cardiologists who use the femoral artery approach will confirm bony landmarks before accessing the artery. This is accomplished by placing a needle or hemostat on top of the groin at the anticipated puncture site and fluroscopically evaluating the position of the tip as it relates to the femoral head. |
| |
FOR AUDIO: Click the Speaker Icon to "unmute" Audio |

| The inguinal ligament usually crosses
the superior edge of the femoral head. In the majority of cases, the common
femoral artery usually bifurcates into the profunda and superficial branches
below the mid portion of the femoral head. The target entry site of the
needle is the superior half of the femoral head and is achieved by controlling
the entrance point, the insertion angle of the needle, and taking into
account the anticipated depth of the artery. Low puncture sites may result in entering one of the bifurcation branches of the common femoral artery. In such cases, compression, post removal of the sheath is more difficult. Also, the incidence of a pseudo-aneurysm and femoral artery thrombosis is slightly increased. Puncture at the arterial bifurcation point may make it more difficult to secure hemostasis with compression or a sealing device, In some cases surgical repair may be needed. A high puncture should be avoided, if possible, because it then becomes difficult to compress the artery against a bony structure and the risk of a retro-peritoneal hematoma is increased. |
| Cardiac Cath 3/6 |